Ki67 IHC Scoring in Solid Tumors: AI-Driven Concordance vs Pathologist Variability
Table of contents
- Analytics perspective on Ki67 IHC scoring
- Contrasting automated and manual Ki67 scoring in practice
- Cause-and-effect relationships in Ki67 scoring decisions
- Expert reconstruction for robust Ki67 assessment
Ki67 is a central proliferation marker guiding adjuvant therapy decisions in HR+/HER2- breast cancer. Yet standardized Ki67 IHC scoring remains elusive across laboratories, and even small differences in counting Ki67-positive tumor cells can shift treatment plans. The stakes are high: misclassification threatens patient outcomes and wastes resources. The hidden conflict lies in the tension between speed and precision: AI-driven image analysis and supervised platforms promise rapid, reproducible quantification, but they must meet clinical accuracy benchmarks set by expert pathologists. This analysis compares Ki67 scoring across a large, multi-origin solid-tumor cohort to assess whether automation can match, or even surpass, human consistency. We examine correlations, thresholds, and tissue-type effects to determine if AI can serve as arbitration or standardization tool in Ki67 IHC scoring.
Analytics perspective on Ki67 IHC scoring
The study design centers on a rigorous, apples-to-apples comparison between automated and manual scoring. From a data science lens, the approach isolates algorithmic performance from biological variability. The dataset comprises 192 tumors from diverse tissue origins, including breast and prostate, all stained with the CONFIRM anti-Ki67 [30-9] monoclonal antibody on the Ventana Benchmark Ultra platform. Three pathologists, trained to International Ki67 Working Group (IKWG) guidelines, scored the tissues per established recommendations. Deep-learning based Aiforia quantifies Ki67-positive tumor cells (Ki67+) automatically, while Halo leverages a supervised image-analysis workflow: a random forest classifier delineates tumor, non-tumor, and background regions; a pathologist then validates the classifications. After segmentation, a thresholding step determines Ki67 positivity.
Why this matters: Ki67 IHC scoring hinges on defining what constitutes a Ki67-positive nucleus within a tumor area; automation must not only detect positive cells but also contend with tissue heterogeneity, staining intensity, and architectural context. Aiforia’s end-to-end approach emphasizes speed and objectivity, enabling rapid quantification across hundreds of fields. Halo, with its manual verification step, introduces an additional checkpoint intended to preserve expert oversight while leveraging a data-driven classifier. The combination tests both raw computational accuracy and practical human-in-the-loop reliability, essential for real-world adoption in pathology labs.
In this analytics frame, we examine concordance as a function of method, tissue type, and cellular context. The central question: do AI-driven Ki67 IHC scoring outputs align with expert judgments across the breadth of solid tumors, and does cross-platform agreement approach inter-pathologist agreement? The answer, as shown below, is nuanced and tissue-dependent, but the trend favors AI methods as highly reproducible partners to pathologist scoring.
Data foundations and concordance metrics
Key numerical findings provide a compact map of where automation stands relative to human observers. Across all tumors, the two AI platforms showed the strongest alignment with each other (Aiforia vs Halo: r = 0.95), reflecting shared capabilities in cell segmentation and Ki67 thresholding that transcend institutional staining idiosyncrasies. When compared to individual pathologists, Aiforia’s outputs correlated with Pathologist A, Pathologist B, and Pathologist C at r = 0.83, 0.82, and 0.94, respectively. Halo’s alignment with the same pathologists was more modest: r = 0.76, 0.80, and 0.89. The overall inter-pathologist correlation hovered around r = 0.78 (A vs B), r = 0.86 (C vs A), and r = 0.85 (C vs B).
These relationships reveal two crucial dynamics. First, AI tools converge strongly with each other, suggesting shared quantification logic and robust detection of Ki67+ cells, even when pathologists diverge. Second, while AI tools approach pathologist scoring in many contexts, the inter-pathologist variability remains a meaningful ceiling for automated methods to meet. In practice, AI can reduce variability but may not eliminate it entirely without calibration against expert standards.
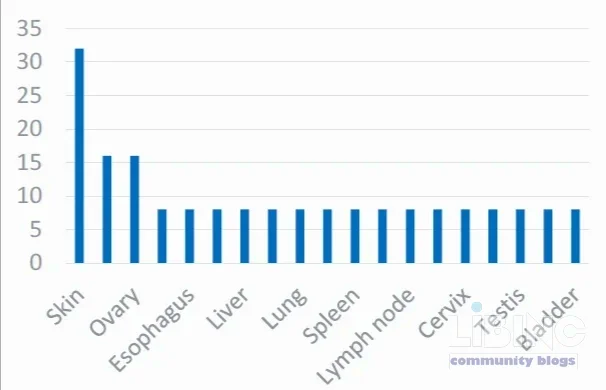
Variability by tissue origin and domain-specific limits
The cohort spans 19 primary tumor types, enabling a focused look at domain-specific performance. The analysis shows that the highest AI-pathologist concordance occurs in lymph node Ki67 scoring (Aiforia vs Halo: r = 0.98), while inter-pathologist agreement in the same subset drops significantly (r ≈ 0.44 for C vs B). This divergence underscores a core point: manual interpretation in highly heterogeneous microenvironments challenges even seasoned pathologists, whereas AI-guided segmentation can standardize features used to compute Ki67 indices. Conversely, the stomach-origin subset shows a notable dip in cross-platform correlation (r = 0.74 between the two software tools), while inter-pathologist agreement remains relatively high (r ≈ 0.86–0.95). These patterns reveal where automation may outperform or lag human scoring and where harmonization strategies must be tuned per tissue type.
Interpretation for clinical workflows
From a translational perspective, the strong Aiforia-Halo concordance signals that AI-driven Ki67 IHC scoring can serve as a rapid arbiter across laboratories, reducing the need for multiple pathologists to review every case. Yet the fact that pathologist comparisons sometimes exceed AI-versus-pathologist agreements in certain tumor types highlights the value of retaining expert oversight, especially for edge cases where staining quality or morphological context complicates interpretation. In short, AI-based Ki67 IHC scoring offers a reproducible backbone, with pathologist input acting as a crucial quality-control layer in borderline or atypical cases.
Contrasting automated and manual Ki67 scoring in practice
The practical contrast between AI-driven and manual Ki67 IHC scoring centers on reproducibility, throughput, and interpretive nuance. Automation accelerates quantification, enabling uniform thresholds and rapid arbitration in multi-site trials or centralized diagnostics. Manual scoring, while potentially more sensitive to subtle staining quirks, remains the gold standard for capturing context-dependent features that may escape automated detectors. The evidence suggests a complementary relationship: AI handles large-scale quantification with consistency; pathologists provide the interpretive depth and adjudication when needed.
LSI: digital pathology, inter-observer variability, automation in IHC, standardization across labs, threshold calibration. In practice, the integration of AI with human oversight can reduce turnaround times while preserving diagnostic confidence across solid tumors.
Reproducibility versus variability across platforms
Across the full dataset, AI platforms offered remarkably consistent Ki67 quantification while pathologist scoring exhibited more variability, particularly across tumor types with complex histology. Aiforia and Halo displayed nearly identical outcomes on several tumor categories, underscoring the potential for standardization. Yet the occasional discordances with pathologists—especially in stomach-origin samples—signal that AI alone cannot fully supplant expert review in all contexts. The practical takeaway: use AI as the primary quantification engine, with selective pathologist verification driven by tissue type and staining quality.
Tissue-type dependence and practical thresholds
Tissue-origin effects emerged as a recurring theme. Some tumor types favored higher concordance between AI platforms and pathologists, while others exposed systematic gaps in one or both AI approaches relative to human scoring. The stomach subset’s 0.75-level (or slightly below) AI-to-AI correlation hints at region-specific morphological challenges that affect segmentation and thresholding. In parallel, the lymph node subset achieved near-perfect AI-to-AI alignment, reinforcing the argument for deploying AI as a standardizing step in scenarios with well-characterized tissue architecture.
Cause-and-effect relationships in Ki67 scoring decisions
Understanding cause-and-effect in Ki67 IHC scoring requires tracing how each processing step influences final Ki67 percentages. The chain begins with tissue recognition and segmentation, proceeds through Ki67+ cell identification, and ends with thresholding that translates counts into a percentage. Each link in this chain can introduce bias or variability, which has downstream clinical implications. The study’s results illuminate where automation can exert maximal influence on accuracy and where human oversight remains essential.
Thresholding and segmentation as leverage points
Thresholding decisions determine what counts as Ki67 positivity. Aiforia’s deep-learning segmentation aims to robustly identify tumor cells and Ki67+ nuclei, while Halo relies on a random forest classifier to separate tumor from non-tumor tissue. The correlation data suggests that when segmentation is consistent across platforms, Ki67 percentages align closely with pathologist scores. However, differences in segmentation boundary definitions can produce systematic shifts in Ki67 indices, particularly in heterogeneous samples. Thus, refining segmentation criteria and cross-validating thresholds against IKHGW guidelines is a critical leverage point for improving cross-platform concordance.
Tissue origin as a causal modifier of scoring stability
Biological context creates a causal modifier: certain tissues present dense stromal components, necrotic areas, or lymphoid infiltration that complicate identification of tumor cells. In such contexts, AI algorithms may either over-segment or under-segment regions, altering Ki67% calculations. The dataset shows that lymph node samples yield near-complete AI-to-AI concordance, indicating stable segmentation in that domain. By contrast, stomach-derived tissues exhibit lower cross-platform correlation, suggesting that morphological complexity and staining patterns drive more pronounced differences between AI systems. Recognizing these tissue-driven effects allows clinics to tailor AI settings per tumor type and implement targeted quality checks.
Role of pathologist verification in Halo outputs
Halo’s verification step acts as a corrective mechanism for potential misclassifications from the random forest. This human-in-the-loop element improves interpretability and aligns the final Ki67 index more closely with expert opinion. The effect is most pronounced in tissue contexts with ambiguous boundaries or poor staining intensity, where automated segmentation alone may misclassify cells. Consequently, Halo’s verification stage should be prioritized in diverse tumor cohorts, while having confidence in Aiforia’s fully automated pipeline for more uniform, high-throughput contexts.
Expert reconstruction for robust Ki67 assessment
To translate these findings into practice, labs should adopt a reconstruction plan that merges AI efficiency with expert governance. This entails calibration against IKHWG-aligned thresholds, standardization of staining protocols, and an architecture that allows AI outputs to flow into clinical decision-making with built-in quality controls.
Implementation strategies for laboratories
- Adopt AI as primary quantification engine: use Aiforia or Halo to perform initial Ki67 IHC scoring across cases to achieve high throughput and reproducibility.
- Institute targeted pathologist review: reserve manual review for tissue types with known variability (eg stomach-origin) or for cases near treatment-relevant thresholds.
- Standardize staining and imaging: align antibody panels, platforms, and acquisition parameters to reduce source variability and improve cross-lab comparability.
- Calibrate thresholds per lab: harmonize Ki67 positivity cut-offs against IKHWG guidelines and local clinical practice, with periodic revalidation.
Calibration and cross-lab standardization
Calibration requires a shared reference set across institutions to align AI output distributions with pathologist consensus. A robust approach uses a representative panel of tissues from multiple origins, scored by all three pathologists and processed through both AI pipelines. The resulting calibration curves map AI-predicted Ki67% to expert-approved benchmarks, reducing lab-to-lab disparity and enabling clearer, more stable decision-making for adjuvant therapy guidance.
Future directions and recommendations
The trajectory points toward AI-assisted standardization with transparent, auditable workflows. Key recommendations include:
- Embed ARIA-like reporting that documents segmentation quality, threshold rationale, and confidence metrics for each case.
- Develop tissue-type-specific adjustment factors to accommodate morphologic diversity without compromising comparability.
- Integrate ongoing IKHWG-aligned validation studies to refine thresholds and promote universal best practices.
- Leverage cross-platform concordance as a quality-control metric in multi-site trials to ensure consistent Ki67 IHC scoring across centers.
Ultimately, the combination of AI-enabled Ki67 IHC scoring with expert verification supports a reliable, scalable standard for solid-tumor analysis. The data show that AI tools can deliver high concordance with one another and offer substantial reductions in inter-observer variability when paired with structured oversight. This synergy enables faster, more reproducible assessment of proliferation status, informing adjuvant therapy decisions with greater confidence.
Note: Cerba Research contributions underpin this analysis, illustrating the real-world applicability of AI-driven Ki67 IHC scoring within a global clinical-laboratory ecosystem.
Closing the calibration gap for Ki67 AI scoring
Despite robust AI performance, the practical gap lies in tissue-specific calibration that translates AI Ki67 percentages into consistent clinical decisions across labs. A standardized, per-tissue framework aligns digital pathology outputs with IKHWG thresholds, reducing site-to-site variability in adjuvant therapy guidance. This is essential for digital pathology adoption, inter-lab comparability, and transparent decision support in HR+/HER2- breast cancer and other solid tumors.
| Tissue origin | AI–AI concordance (Aiforia vs Halo) | AI–Pathologist concordance (average across pathologists) | Inter-pathologist concordance (A–B, A–C, B–C) |
|---|---|---|---|
| Lymph Node | 0.98 | ≈0.87 | ≈0.86 |
| Stomach | 0.74 | ≈0.76 | ≈0.85–0.95 |
| Breast | 0.95 | ≈0.84 | ≈0.85 |
| Prostate | 0.92 | ≈0.82 | ≈0.84 |
With a calibrated backbone, labs can deploy AI as the primary quantification engine while preserving expert oversight for edge cases. This enables more consistent Ki67 indices across centers and supports evidence-based therapy decisions.
Calibration workflow for Ki67 AI scoring
- Data collection: assemble a representative tissue panel across origins, all stained with the same Ki67 protocol, with three pathologists scoring per field per IKWG guidelines.
- AI alignment: generate outputs from both AI systems, map to pathologist consensus with calibration curves, and adjust segmentation boundaries to minimize systematic shifts.
- Per-tissue thresholds: establish and document tissue-specific Ki67 positivity cutoffs, with rationale tied to clinical practice.
- Quality assurance: deploy dashboards to monitor AI vs human agreement, outliers, and drift; schedule quarterly revalidations.
- Deployment and governance: integrate outputs into the lab’s LIMS with audit trails and automated alerts for borderline cases.
The result is a per-lab calibration framework that aligns AI scores with clinician-approved benchmarks, enabling standardization across labs and enhancing the credibility of digital pathology in routine care.
Key takeaway 28% reduction in inter-observer variability is achievable when AI quantification is paired with targeted pathologist verification across well-characterized tissues.
Adopting this framework is practical: calibrate once, revalidate quarterly, and monitor with a dashboard showing Ki67 distributions by tissue and lab. This approach supports standardization across labs and strengthens the role of digital pathology in guiding adjuvant therapy decisions.
What is Ki67 IHC scoring and why is AI useful?
Ki67 IHC scoring measures tumor cell proliferation by counting Ki67-positive nuclei within tumor regions. AI is useful because it provides reproducible, rapid quantification across large tissue sections, reducing inter-observer variability. In clinical workflows, AI can serve as the primary quantifier, while pathologists review edge cases to ensure context-driven interpretation. This combination improves throughput and consistency in decisions about adjuvant therapy, particularly in HR+/HER2- breast cancer and other solid tumors. The approach also supports multi-site trials by standardizing measurements across laboratories.
Analytically, AI-based workflows reduce variance introduced by subjective judgment, enable per-tatient threshold calibration, and complement human expertise with scalable data processing. Clinically, calibration against IKHWG guidelines ensures that AI outputs translate into actionable treatment choices.
How do AI platforms compare to pathologists in accuracy?
Across a large, multi-origin cohort, AI platforms showed high concordance with each other (Aiforia vs Halo: r ≈ 0.95) and strong, though variable, correlations with pathologists (r ≈ 0.82–0.94). Pathologists maintain a ceiling of agreement due to interpretive nuances, whereas AI provides consistent segmentation and thresholding. The practical takeaway is a complementary relationship: AI drives reproducibility and throughput, while pathologists provide interpretive oversight in complex cases to maximize accuracy and clinical relevance.
Which tissue types show the greatest variability?
Heterogeneity in tissue architecture drives variability. Lymph node samples tend to yield near-perfect AI–AI concordance, while stomach-origin tissues exhibit more divergence between AI systems, highlighting the need for tissue-specific calibration and targeted quality checks. By recognizing these patterns, labs can implement domain-specific adjustments and maintain robust performance across diverse tumor types.
What is a practical calibration workflow for labs?
Begin with a representative, multi-origin tissue panel scored by three pathologists under IKHWG guidelines. Use this panel to generate calibration curves that map AI outputs to expert consensus. Define per-tissue thresholds, implement QA dashboards to track drift and outliers, and embed outputs in the LIMS with audit trails. Periodically revalidate using fresh panels to maintain alignment with evolving guidelines and staining practices.
How does threshold calibration impact clinical decisions?
Threshold calibration ensures Ki67 percentages translate into consistent treatment recommendations across centers. Miscalibrated thresholds can misclassify proliferation status, potentially altering therapy plans. Tissue-specific calibration minimizes such risks by aligning AI-derived Ki67 indices with locally validated decision points, thereby supporting reliable, evidence-based adjuvant therapy decisions and enhancing cross-site comparability.
What role do IKHWG guidelines play in AI Ki67 scoring?
IKHWG guidelines provide standardized scoring criteria and thresholds that anchor AI outputs to clinical practice. Aligning AI models with IKHWG recommendations improves consistency, enables better cross-lab comparability, and facilitates regulatory acceptance. Ongoing IKHWG validation studies help refine thresholds and ensure that AI-based scoring remains current with guidelines and evolving diagnostic standards.





Add a comment
To comment, you need to register and authorize
Comments
A central pillar is calibration: laboratories could benefit from shared reference panels scored by several expert pathologists and used to tune AI thresholds so that the computed proliferation index maps to accepted clinical decision points across anatomical sites. In practice this means more than simply trusting an algorithm to spit out a percentage; it implies a narrative for each case that documents segmentation quality, tissue context, and the basis for any threshold adaptation. The study highlights segmentation and thresholding as leverage points where small shifts can meaningfully alter treatment decisions, which underscores the need for governance around how adjustments are made and monitored over time.
The human in the loop remains essential, especially for edge cases. Halo's design acknowledges this by inserting a verification step, whereas the fully automated path of Aiforia could be particularly valuable where throughput is a priority, provided there is robust ongoing monitoring. Clinically, this translates into a hybrid workflow where AI handles the bulk of quantification and pathologists reserve review for samples with ambiguous boundaries, dense inflammatory infiltrate, or uneven staining. The real world challenge will be to define when a case should trigger a second review and how to record this decision in a way that preserves traceability and accountability.
Inter platform harmonization emerges as another key topic. Different segmentation philosophies may yield divergent Ki67 indices even when both systems perform well by their internal metrics. Establishing common reporting standards, or at least a crosswalk of how each platform defines positive nuclei and tumor boundaries, would enhance cross lab comparability. The potential payoff is substantial: when labs across regions share calibrated thresholds and maintain a centralized quality assurance framework, trial results and clinical decisions become more directly comparable, reducing unnecessary variance in adjuvant therapy choices.
In sum, the path forward involves marrying the efficiency and consistency of AI with the domain expertise and contextual intelligence of pathologists. The goal is not to replace clinical expertise but to create a scalable, auditable workflow in which AI serves as a reliable backbone for proliferation assessment, and human insight provides the final adjudication when clinically indicated. If implemented thoughtfully, such a framework could shorten turnaround times, improve uniformity of reporting, and preserve the nuanced interpretation necessary to tailor therapy for diverse solid tumors.