Multiplex immunohistochemistry for tumor microenvironment profiling: ROI-based analytics across tissues
Table of Contents
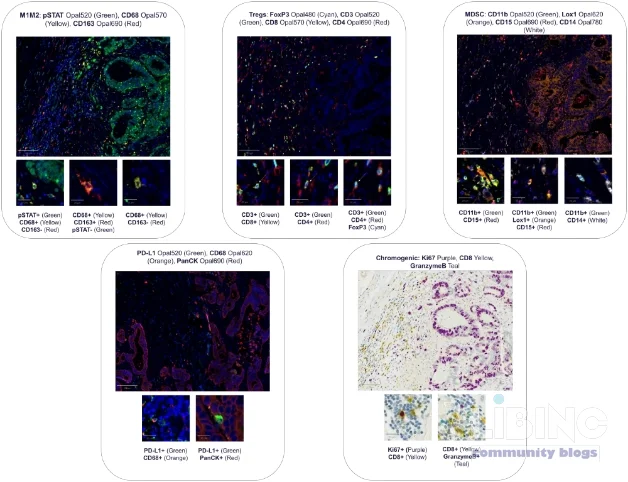
Main concept the ability to profile the tumor microenvironment (TME) through multiplex immunohistochemistry (mIHC) allocation of multiple markers within a single tissue section. This approach, particularly when paired with ROI mapping and quantitative image analysis, yields actionable insight into immune subsets, functional states, and spatial interactions that drive pro- or anti-tumor dynamics. The poster under discussion demonstrates how two automated staining platforms, Leica Bond Rx and Roche Discovery Ultra, combined with Akoya Opals for fluorescence and Roche Chromogens for chromogenic readouts, enable robust cross-tissue profiling in normal and tumor tissues from pancreas, lung, and colon. The aim is to translate rich cellular phenotypes into precise immunotherapy concepts while maintaining analytical rigor.
In this analysis, four regions of interest (ROIs) per block were chosen to anchor cross-sample comparisons. A board-certified pathologist mapped the ROIs to analogous multiplex panel slides to ensure tissue context remained consistent. Images were captured and processed in a workflow that avoids spectral deconvolution, with quantification performed by HALO (Indica Labs). The resulting metrics capture both absolute abundance and phenotype composition within and across ROIs, enabling an apples-to-apples comparison with whole-tissue measurements through matched-pair analysis in JMP. The upshot is a workflow that blends high-content imaging with disciplined statistics to reveal how spatial organization shapes immune surveillance and tumor immunobiology.
Analytics-driven ROI-based mIHC workflow for immune profiling
The analytic spine of the poster rests on a carefully designed mIHC strategy that leverages two automated staining platforms to maximize throughput and reproducibility. The Bond Rx system contributes robust, automated staining chemistry for chromogenic and fluorescent readouts, while the Discovery Ultra delivers parallel staining capacity for multiplex panels with high sensitivity. The detection chemistries deployed include Akoya Opals for fluorescence and Roche Chromogens for chromogenic assays. This combination preserves signal integrity while enabling multi-parameter assessment in the same tissue context.
- The assay design prioritizes quantification of melting points in the TME: single-marker positivity (for example CD8, CD68, PD-L1) and derived phenotypes (such as macrophage subsets, activated cytotoxic T-cells, and regulatory T-cells). This dual granularity—cell counts and functional state classification—supports capturing both abundance and activity within spatial niches.
- ROI mapping anchors tissue reference frames by aligning four ROIs per block with analogous panel slides. The strategy mitigates sampling bias and supports cross-tissue comparability by preserving architectural context within each ROI.
- Image capture and analysis rely on a validated pipeline that does not require spectral deconvolution. HALO quantification provides metrics across ROIs, distinguishing combined marker levels and phenotype-level readouts from any whole-tissue data harvested from the same slide.
- Matched-pair analysis in JMP directly contrasts ROI-based metrics with whole-slide measurements for the same sample. This design tests the core assumption that well-chosen ROI captures reflect the tissue’s global immune milieu.
The analytics reveal several critical dynamics. First, the panels demonstrate exceptional versatility, distinguishing immune profiles in healthy versus tumor tissues across pancreas, lung, and colon. Second, the approach supports both cellular abundance and spatial organization metrics, enabling a multi-dimensional view of TME architecture. Third, the ROI-based workflow yields quantitative continuity with whole-tissue data, reinforcing the biological relevance of ROI selections and supporting cross-tissue comparisons that would be difficult with single-parameter readouts alone.
From an analytical standpoint, the ROI-centric design answers a central question: why do certain immune landscapes emerge in a given tissue, and how do those landscapes relate to tumor biology? The answer lies in combining quantitative single-marker data with phenotype delineations that reflect functional states and interactions within spatially defined niches. The integration of pathology-grade ROI mapping with high-resolution imaging and rigorous statistics creates a robust framework for identifying immuno-oncology biomarkers that are both tissue-context aware and transferable across tumor indications.
Key analytic elements
- Spatially informed phenotyping: deriving functional states from marker co-expression patterns within specific microenvironments.
- Cross-platform harmonization: reconciling staining outputs across Bond Rx and Discovery Ultra to ensure consistent quantitation.
- Quantitative ROI vs whole-tissue metrics: directly evaluating the representativeness of ROI-derived data for broader tissue contexts.
- Statistical backbone: matched-pair comparison, variance assessment, and cross-case consistency checks to validate ROI strategies.
ROI-based versus whole-tissue quantification: contrasts across tissues
ROI-based quantification is not a simplification—it is a principled approach that acknowledges tissue heterogeneity while delivering scalable, comparable data. Across pancreas, lung, and colon, the multiplex panels reveal distinct immune landscapes in normal versus tumor tissue. This differentiation is not solely about cell density; it encompasses spatial organization, such as clustering of activated effector cells near tumor borders or the accumulation of suppressive macrophages within stromal niches. The ability to quantify both single-marker positivity and derived phenotypes enables a richer interpretation of immune contexture than either metric could provide alone.
- Cross-tissue distinctions emerge when comparing ROIs from normal pancreas to pancreatic tumor tissue, lung parenchyma to malignant lesions, and colon mucosa to colorectal tumors. These contrasts illuminate tissue-specific immunobiology and potential therapeutic vulnerabilities.
- Phenotype-level granularity differentiates macrophage subsets (for example, M1-like vs M2-like states) and T-cell functional status (eg, activated cytotoxic T cells, exhausted phenotypes, regulatory T cells), highlighting how cellular function intertwines with spatial context.
- Spatial metrics such as proximity to tumor cells, proximity to vasculature, and neighborhood density offer complementary readouts that refine risk stratification and biomarker signatures.
- Matched-pair validation demonstrates that ROI-derived metrics closely track whole-tissue measurements, reinforcing confidence in ROI-based conclusions and enabling robust cross-tissue comparisons without harvesting entire slides.
The ROI-based approach yields a practical, scalable framework for cross-tissue immunoprofiling. It recognizes that tumor and immune cells do not exist in isolation but in spatially organized ecosystems. By preserving tissue architecture while enabling high-throughput analysis, this workflow helps researchers translate descriptive observations into actionable immuno-oncology biomarkers and therapeutic hypotheses.
Cause and effect: implications for biomarker strategies
What follows from the ROI-centric mIHC workflow is a set of causal inferences about biomarker discovery and test design. Precisely mapped ROIs, aligned across platforms and tissue types, reduce sampling bias and strengthen the link between observed immune states and clinical phenomena. The ability to quantify single-marker positivity in tandem with phenotypic assignments yields biomarker panels that are both interpretable and mechanistically informative.
- Biomarker stability: ROI-based quantification reduces stochastic variation inherent in small biopsy samples, supporting more reproducible biomarker readouts across cohorts and laboratories.
- Functional relevance: derived phenotypes provide mechanistic insight into how immune cells operate within specific TME niches, informing strategies to bolster anti-tumor immunity or to counteract immune suppression.
- Spatially aware signatures: incorporating spatial relationships into biomarker panels improves predictive value for immunotherapy response and resistance mechanisms.
- Cross-tissue portability: matched-pair data empower cross-tumor comparisons, enabling pan-cancer biomarker panels that respect tissue-specific biology while preserving a shared analytic framework.
In practice, this means biomarker development moves beyond mere counts of immune cells. It embraces the architectural arrangement of the TME, the functional states of key players, and their interactions with tumor cells. The result is a biomarker strategy that is both biologically grounded and pragmatically scalable, increasing the likelihood that identified markers translate into clinically meaningful immuno-oncology tools.
Expert reconstruction: implementing mIHC workflows for precision immunotherapy
Translating the demonstrated workflow into routine practice requires deliberate operational and analytic design. The following reconstruction synthesizes the poster insights into an actionable blueprint for laboratories pursuing precision immunotherapy programs.
- Platform standardization: adopt compatible staining workflows across Bond Rx and Discovery Ultra to minimize run-to-run variability. Harmonize detection chemistries and imaging conditions to support consistent quantification of markers and phenotypes in all tissue types under study.
- Panel design and validation: tailor panels to quantify key immune subsets and functional states while preserving cross-panel compatibility. Validate marker combinations for reliable co-expression analysis and robust ROI-level readouts.
- ROI selection strategy: implement predefined criteria for ROI placement based on tissue architecture and prior biological knowledge. Include a diverse set of ROIs per block to capture regional heterogeneity and to maximize representativeness.
- Image analysis and statistics: rely on an internally validated HALO workflow for quantification, followed by JMP-based matched-pair analyses to compare ROI and whole-tissue data. Document all mappings between ROIs and panels to ensure reproducibility.
- Cross-tissue comparability: establish reference datasets that enable cross-tissue and cross-tumor comparisons. Use ROI-based metrics as a bridge between tissue-specific biology and universal immuno-oncology concepts.
- Operational readiness: leverage Cerba Research capabilities to scale testing across a global network, integrating histopathology, flow cytometry, bioanalysis, and sequencing to support comprehensive biomarker programs in Virology, Immunology, Oncology and Cell & Gene Therapy.
Future refinements may include expanding the use of high-plex imaging to additional tumor indications, integrating spatial transcriptomics for multi-modal cross-validation, and developing automated quality control routines that detect platform-specific drift without compromising throughput. The overarching goal is a robust analytical framework that consistently informs precision immunotherapy design and evaluation across tissues and indications.
Practical takeaways for labs
- Maintain spectral integrity by selecting detection chemistries that minimize bleed-through and allow clean delineation of cell phenotypes within ROI contexts.
- Preserve ROI integrity through rigorous mapping between ROI slides and panel slides to maintain consistent tissue context for quantitative comparisons.
- Prioritize spatial relationships when interpreting biomarker panels, as proximity and neighborhood effects can dramatically influence functional state assignments.
- Embed statistical validation in daily workflows, employing matched-pair analyses to quantify the fidelity of ROI-based inferences to whole-tissue realities.
The integrated workflow described here positions multiplex immunohistochemistry as a dynamic, evidence-driven engine for immune profiling. By combining automated staining platforms, high-resolution imaging, ROI mapping, and rigorous quantitative analysis, researchers gain a powerful lens on how immune ecosystems shape tumor behavior and treatment outcomes. This is not merely data collection; it is a disciplined strategy to convert complex tissue biology into actionable precision immunotherapy insights.
In closing, multiplex immunohistochemistry, when deployed with ROI-based analytical rigor across normal and tumor tissues, delivers a robust analytical framework for immuno-oncology biomarkers. The cross-platform, cross-tissue approach enables detailed spatial and functional mapping of immune contexts, laying the groundwork for more accurate patient stratification and more effective immunotherapies. The pathway from deep tissue characterization to clinical impact is clearer, more scalable, and more scientifically grounded than ever before.
Closing the measurement fidelity hole
Even when ROI-based mIHC yields cross-tissue insights, a formal layer for normalization across platforms and tissues is essential to sustain consistency. Variations in staining intensity, imaging exposure, and analyst calibration can shift marker readouts. A practical normalization approach uses internal reference cells (for example, epithelial or endothelial populations) and a minimal set of platform controls processed in parallel to calibrate signal scales before comparison. Compute marker-positive cells per unit area and express them as ratios to stable references within each ROI. This simple step reduces run-to-run and site-to-site drift, strengthening biological interpretation across pancreas, lung, and colon in both normal and tumor contexts. Spatial biology, tissue architecture, and immuno-oncology biomarkers gain reliability when normalization is explicit and transparent.
ROI Sampling Grid
| ROI | Tissue | Panel | Purpose | Notes |
|---|---|---|---|---|
| ROI-1 | Pancreas normal | A | Baseline reference | Epithelial reference |
| ROI-2 | Lung tumor | B | Immune hotspot | Proximity to tumor cells |
| ROI-3 | Colon tumor | A | Functional states | Macrophage-rich niche |
| ROI-4 | Pancreas tumor | C | Spatial interaction | Peri-vascular niche |
Caption: ROI sampling grid for cross-tissue benchmarking
Another layer of rigor comes from quality control and cross-platform alignment. Track signal-to-noise ratios, bleed-through, and dynamic range; implement daily QC checks and weekly cross-lab benchmarks to detect drift early. These controls enable ROI-derived readouts to mirror whole-tissue measurements, supporting cross-tissue immunoprofiling that is robust enough for multi-site studies. In practice, labs should document normalization steps, ROI placement criteria, and concordance metrics so that data are reproducible across cohorts and sites. This explicit transparency is essential for translating biomarker signatures into actionable immuno-oncology insights.
In addition, reporting guidelines should include ROI criteria, normalization methods, and concordance metrics. This clarity fosters reproducibility and enables broader adoption of ROI-based strategies as a standard approach in multi-indication immuno-oncology programs.
ROI workflow steps
- Define ROI criteria anchored in tissue architecture and prior biology
- Include diverse regions to capture regional heterogeneity
- Align ROIs across panels to preserve context
- Standardize staining and imaging to minimize platform drift
- Harmonize detection chemistries and imaging settings
- Monitor spectral bleed-through and dynamic range
- Quantify markers in a robust analytics workflow (single-marker and phenotype-level readouts)
- Compute cells per mm2 and phenotype composition per ROI
- Apply quality controls and normalization factors
- Perform matched-pair cross-tissue analysis to assess representativeness
- Compare ROI-derived metrics with whole-tissue measurements
- Evaluate concordance across tissues and indications
Adopting these steps improves consistency and enables ROI-based outcomes to mirror broader tissue biology, laying a solid foundation for cross-tissue immuno-oncology programs.
What is ROI-based multiplex immunohistochemistry and why use ROI-based analysis?
ROI-based multiplex immunohistochemistry (mIHC) focuses measurements on predefined tissue regions that capture the essential architecture and function of the tumor microenvironment, enabling consistent comparisons across samples. This approach reduces sampling bias and supports density estimates that reflect both abundance and spatial context, which are critical for immunotherapy biomarker discovery. By anchoring analysis to well-characterized ROIs, laboratories can generate reproducible readouts that are comparable across platforms, tissues, and cohorts. The method also highlights localized microenvironments such as tumor borders or stromal niches, where immune cells exert strong influence on outcomes.
Analytically, ROI-based readouts enable simultaneous assessment of cell counts and functional states, preserve tissue context, and facilitate cross-tample standardization. When combined with matched-pair analyses, the approach translates to robust biomarker panels with practical value for predictive modeling and therapeutic decision-making.
How does ROI-based analysis compare to whole-tissue quantification, and what indicates reliability?
ROI-based analysis offers a scalable, tissue-context aware alternative to complete tissue quantification. Reliability improves when ROIs are representative, when normalization aligns scales across runs, and when concordance with whole-tissue measurements is demonstrated via matched-pair analyses. Key metrics include correlation coefficients between ROI-derived and whole-tissue readouts, within-sample variance, and consistency across tissues. These elements collectively increase confidence that ROI results reflect the biology of the entire tissue domain and are suitable for cross-tissue biomarker development.
Which biomarkers and phenotypes are most informative in ROI-based profiling?
Informative markers include lineage markers (CD8, CD68), activation or exhaustion indicators (Granzyme B, PD-1, TIM-3), and regulatory markers (FoxP3). Phenotypic assignments—such as activated cytotoxic T cells or M1/M2-like macrophages—provide functional context that complements simple cell counts. Spatial readouts, like proximity to tumor cells or vasculature, add predictive value by linking cell state to microenvironmental niches. The goal is to combine abundance with behavior in spatially defined communities to support immunotherapy strategies.
How is cross-platform harmonization achieved across staining platforms?
Harmonization relies on standardizing panels, aligning detection chemistries, and using shared reference controls processed under identical conditions. Calibration steps include parallel runs with the same slides across platforms and the use of internal controls to adjust signal scales. Regular QC checks for bleed-through, dynamic range, and image quality are essential, as is documenting all processing steps so data remain comparable between sites and over time.
What are practical steps to implement ROI-based mIHC in a lab?
Start with a clear ROI strategy and predefined sampling criteria, then establish a cross-platform staining plan with validated panels. Implement a robust image-analysis workflow (marker co-expression, phenotype assignment, ROI-level metrics) and couple it with matched-pair comparisons to whole-tissue data. Maintain a repository of reference slides and a reproducible reporting template that records ROI mappings, normalization factors, and quality metrics. Finally, participate in cross-lab benchmarking to ensure robustness and facilitate broader adoption of ROI-based immunoprofiling across indications.
What limitations should be considered when interpreting ROI-based results?
ROI-based analyses may miss rare cell populations outside selected regions or fail to capture global heterogeneity if ROI coverage is insufficient. Accurate ROI placement hinges on prior tissue knowledge, and normalization can mitigate but not fully remove platform-specific biases. Therefore, ROI findings should be corroborated with whole-tissue data or orthogonal assays when feasible, and results should be interpreted within the context of tissue architecture and sampling density.





Add a comment
To comment, you need to register and authorize
Comments