Actionable Biomarkers in NSCLC: Integrating Targeted Therapies with Immunotherapy Through Immune Contexture Profiling
Targeted therapies for NSCLC increasingly hinge on actionable biomarkers, yet long-term benefit is thwarted by adaptive resistance. Immune checkpoint inhibitors offer selective durable responses, but only in a subset of patients, and optimising who benefits remains elusive. Emerging evidence supports synergy between targeted agents and immunotherapy, especially in tumors bearing rare biomarkers, where singular strategies falter. This analysis examines how actionable biomarkers in NSCLC relate to the tumor immune contexture and what role reflex testing and multiplex immune profiling might play in guiding next-generation combination strategies. By aligning molecular alterations with the surrounding immune landscape, clinicians can move from one-dimensional targeting toward precisely tailored regimens that anticipate resistance and shape durable responses.
Actionable biomarkers in NSCLC: analytics-driven assessment
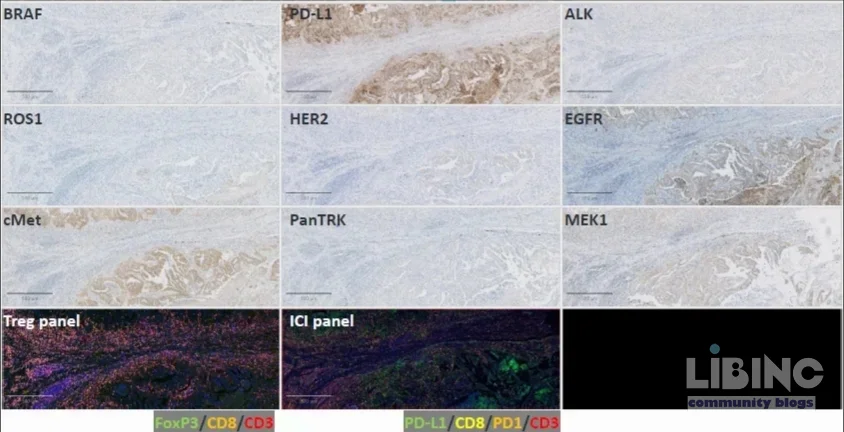
The available evidence base centers on a cohort of 30 NSCLC FFPE samples derived from Cerba Research, designed to screen for druggable and exploratory targets. IHC was employed as a first-pass screen to rapidly identify potential targets and inform reflex testing decisions. In this context, actionable biomarkers in NSCLC show notable heterogeneity: pan-TRK, BRAF, and ROS1 exhibit extremely low staining levels, which complicates reliable interpretation when used as sole determinants of therapy. While around half of cases display focal staining for some targets, none demonstrates the diffuse 2+/3+ ROS1-like pattern required for broad clinical actionability by conventional criteria. These findings underscore a key tension: rarity limits single-modality targeting, yet even diffuse positivity is not guaranteed to translate into clinical efficacy without contextual immune data.
From a data-analytic standpoint, the low prevalence of rare targets stresses the importance of integrating biomarker data with the tumor immune microenvironment (the immune contexture). The cohort reveals that mere presence or absence of a target cannot reliably predict response to targeted therapy in NSCLC without considering immune features. This is where reflex testing becomes crucial: an initial IHC screen flags candidates for deeper evaluation, while subsequent multiplex profiling maps how immune cells, checkpoint molecules, and pathway drivers co-shape therapeutic vulnerability. Actionable biomarkers in NSCLC thus function best when treated as components of an integrated signal rather than standalone binary indicators.
Across the screened samples, several associations emerge that inform both biology and strategy. PD-L1 expression correlates with cMET, MEK1, and EGFR, suggesting convergent signaling axes that may modulate tumor–immune interactions. MEK1+ tumor cells show notable associations with infiltrating immune populations and PD-1 expression, implying that MEK1-related signaling or its inhibition could influence immune surveillance. Conversely, PD-L1 and PD-1+ cytotoxic T-cells do not exhibit a robust direct relationship, reinforcing the practice of evaluating PD-L1 and PD-1 independently when planning ICI-based therapy. These analytic patterns argue for a multilayered diagnostic approach to identify co-activations that predict response or resistance to combination regimens.
Another analytic takeaway concerns the relationship between target expression and cellular phenotypes. HER2 expression appears associated with greater densities of helper and cytotoxic T-cells, consistent with literature suggesting limited responses to PD-1/PD-L1 blockade in HER2-positive NSCLC. This points to a need for alternative immunomodulatory strategies or combination partners beyond PD-1 blockade in HER2-driven contexts. The stable or emergent correlations between PD-1+ cells and specific T-cell subsets (CD3+/CD8+/FoxP3+) across panels indicate that profiling must dissect both cytotoxic and regulatory compartments to predict net immune pressure and potential escape routes. Actionable biomarkers in NSCLC therefore require contextual interpretation within a broader immunologic map rather than isolated marker assessment.
In practical terms, these analytics support a workflow where IHC serves as a fast, cost-effective first screen, followed by reflex testing and multiplex immune profiling to construct a comprehensive biomarker-immune phenotype. The data also align with the principle that predictive modeling benefits from panels that capture both driver alterations and immune contexture, enabling more nuanced predictions of response to ICI-based combinations. The central implication for clinicians is clear: actionable biomarkers in NSCLC gain predictive value only when embedded within a rigorous immune profiling framework that accounts for heterogeneity and pathway crosstalk.
Actionable biomarkers in NSCLC: contrasts between IHC-only screening and multiplex profiling
One of the core contrasts in NSCLC biomarker strategy is between rapid IHC-based screening and deeper multiplex profiling that includes immune contexture. IHC alone delivers speed and convenience, but its sensitivity for rare targets is limited and its predictive value for immunotherapy remains incomplete without immune data. In the Cerba Research cohort, the IHC approach could not reliably classify a substantial fraction of tumors for targeted therapy due to the scarcity of true POSITIVE rare targets and the absence of robust, diffuse staining patterns for ROS1. This limitation exposes a gap between apparent target presence and actual therapeutic opportunity, underscoring the risk of over-reliance on single-modality screens.
Multiplex profiling integrates immune phenotypes with target expression, offering a more nuanced view of tumor biology. The data show that while a minority of cases display detectable targets, the distribution of biomarker positivity across the cohort reveals substantial heterogeneity. This heterogeneity is not merely academic; it translates into practical differences in how patients may respond to combinations of TKIs and ICIs. The tumor immune contexture, captured through multiplex panels, informs the likelihood of synergy or cross-resistance between targeted agents and immune modulation, guiding smarter trial design and patient selection. Actionable biomarkers in NSCLC become powerful when embedded in a profiling framework that links signaling pathways to immune cell densities and functional states.
Reflex testing represents a crucial bridge between the two approaches. When IHC suggests a potential target, reflex testing with more comprehensive assays refines therapy choice and avoids missing opportunities due to false negatives or ambivalent staining. Multiplex immune profiling adds another layer by characterizing T-cell subsets (CD3+, CD8+, FoxP3+), checkpoint expression (PD-1, PD-L1), and other modulators within the microenvironment. These dimensions together enable a more precise patient stratification for ICI-based combinations, especially in tumors with rare biomarker signatures where traditional single-marker rules fail. Actionable biomarkers in NSCLC thus require both the speed of IHC and the depth of multiplex profiling to optimize treatment decisions.
Despite the promise of multiplex profiling, practical implementation must consider cost, tissue availability, and turnaround times. The Cerba dataset demonstrates the value of a staged diagnostic approach: quick initial screening to identify obvious targets, followed by thorough immune-contexture assessment to inform combination strategies. The overall takeaway is that actionable biomarkers in NSCLC are most informative when screened through a two-step process that marries rapid identification with comprehensive immune characterization, thereby improving the predictive accuracy for ICI-based regimens.
Actionable biomarkers in NSCLC: cause-and-effect relationships in biomarker-immune interactions
The relationships observed in the cohort suggest several cause-and-effect implications for therapy design in NSCLC. The strong correlation between MEK1 expression and both immune cell infiltration and PD-1 expression points to a signaling–immune axis that could be exploited therapeutically. In practical terms, MEK1 pathway activity may influence the recruitment or retention of PD-1-expressing T cells within the tumor microenvironment, creating a rationale for combining MEK inhibitors with PD-1 blockade in MEK1-dominant contexts. This is not merely academic; the data imply that altering tumor signaling could reshape the immune milieu to favor effective anti-tumor responses when paired with ICIs. Actionable biomarkers in NSCLC thus become prospective targets for rational combination strategies rather than static targets to be inhibited in isolation.
PD-L1's associations with cMET, MEK1, and EGFR reinforce a theme of pathway convergence shaping immune interactions. Tumors with high PD-L1 may simultaneously harbor co-activated signaling axes that sustain an immunosuppressive milieu or, conversely, render them more amenable to combined targeting. HER2, by contrast, shows an association with greater T-cell densities, suggesting a more inflamed microenvironment that, paradoxically, may not translate into robust responses to PD-1/PD-L1 blockade. This underscores a critical principle: the presence of immune cells does not guarantee benefit from ICIs unless the regulatory signals and co-expressed pathways are harmonized with checkpoint inhibition. Actionable biomarkers in NSCLC therefore require joint consideration of checkpoint status, target pathways, and the broader immune landscape to predict synergy or antagonism in combination regimens.
Another causal insight emerges from the independence of PD-L1 and PD-1+ cytotoxic T-cells. The lack of a strong relationship between these two markers in the dataset reinforces the clinical practice of assessing PD-L1 and PD-1+ populations separately when modeling ICI responses. It also suggests that relying on PD-L1 status alone may be insufficient to predict cytotoxic T-cell function or to anticipate the impact of PD-1 blockade. Consequently, a decision framework for NSCLC should integrate PD-L1, PD-1+, and T-cell subset data to capture the nuanced balance of effector and regulatory forces driving response or resistance. Actionable biomarkers in NSCLC thus reveal a complex causal web where signal transduction, immune checkpoints, and cellular phenotypes interact to shape therapeutic outcomes.
Finally, the relationship between target expression and immune contexture highlights that biomarker co-expression patterns matter more than single markers. The observed ties between MEK1, PD-L1, and immune populations illuminate potential synergistic mechanisms, while the absence of a universal PD-L1–immune cell correlation signals the perils of one-size-fits-all strategies. These causal dynamics argue for dynamic, phenotype-driven treatment design: use multiplex contextures to decide when to pair MEK inhibitors with ICIs, when to prioritize alternative immunomodulators, and when to apply reflex-targeted approaches only after confirming cooperative signaling. Actionable biomarkers in NSCLC thus guide not only what to target, but how to orchestrate the sequence and combination of interventions for durable control.
Actionable biomarkers in NSCLC: expert reconstruction for future strategies
The Cerba Research data illuminate a path forward for aligning diagnostic workflows with therapeutic ambitions in NSCLC. IHC screening remains a valuable first line for rapid insight into potential targets, but its limitations for rare biomarkers require reflex testing and, increasingly, multiplex immune profiling to capture the full biological context. The most promising horizon lies in pairing actionable alterations with immune contexture, enabling rational combination strategies that address both tumor-intrinsic drivers and tumor-extrinsic immune constraints. In practice, actionable biomarkers in NSCLC should be treated as components of an integrated decision framework rather than isolated signals, with diagnostic pathways designed to reveal co-activated pathways and corresponding immune states.
Concrete recommendations emerge from the analytics and correlations observed. First, implement a two-step diagnostic workflow: initial IHC for speed, followed by reflex, multiplex profiling to map the tumor immune contexture and target co-dependencies. Second, tailor combination strategies to phenotype: consider MEK1-directed approaches in tumors with concurrent PD-1+ T-cell infiltration, where MEK1 inhibition may lower immune escape barriers and improve ICI efficacy; in contrast, HER2-high tumors may require immunomodulatory additions beyond PD-1 blockade due to their distinct immune milieu. Third, design trials that stratify patients by both target expression and immune contexture, enriching for cohorts most likely to benefit from targeted-plus-immunotherapy regimens. Fourth, invest in standardized biomarker panels and cross-lab data harmonization to enable robust meta-analyses and scalable clinical implementation. Actionable biomarkers in NSCLC, when integrated with immune profiling, can drive more precise, durable responses and help anticipate resistance trajectories rather than merely reacting to them.
From a practical perspective, the expert reconstruction emphasizes reflex testing and multiplex panels as core elements of the cancer-testing toolkit. The ultimate aim is to translate the observed associations into actionable clinical pathways that improve patient selection for combination regimens, reduce unnecessary exposure to ineffective therapies, and accelerate the development of biomarker-informed protocols. As the field evolves, larger, multi-institutional datasets will be essential to validate these patterns and refine predictive models that translate into real-world gains for NSCLC patients. Actionable biomarkers in NSCLC thus become catalysts for more deliberate, data-driven, and patient-centered care that blends molecular targeting with immune modulation.
Notes: This analysis builds on data from Cerba Research and the broader literature on NSCLC biomarker testing, targeted therapy, and immunotherapy. Where figures or tables were referenced in the source material, they are interpreted here to highlight practical implications for reflex testing, multiplex profiling, and combination strategies.
Conclusion: A unified approach that combines robust biomarker testing with comprehensive immune contexture profiling offers the most promise for refining NSCLC treatment. By recognizing the limits of single-modality screens and embracing integrated analytics, clinicians can better anticipate resistance, select appropriate partners for immunotherapy, and design trials that translate into meaningful patient outcomes. Actionable biomarkers in NSCLC, understood through both molecular and immune lenses, set the stage for truly personalized combination regimens.
The Cerba Research data illuminate a path forward, but a practical, standardized workflow is still needed to translate complex biomarker-immune signals into concrete treatment decisions.
| Aspect | IHC-only screening | Multiplex profiling | Clinical implication | Notes |
|---|---|---|---|---|
| Target prevalence | Rare, often focal | Contextual: targets plus immune data | Guides reflex testing decisions | Risk of false negatives; requires confirmation |
| Actionability | Often limited to strong, diffuse positives | Enhanced with immune markers | Supports targeted-immunotherapy combos only with context | Integrate with immune profiling for reliability |
| Turnaround time | Fast for screening | Longer; higher cost | Better patient stratification; informs trials | Balance speed with data depth |
| Predictive value | Limited for ICI without immune data | Higher when combined with contexture | Enables rational combos; reduces futile trials | Requires standardized panels |
Figure: A two-track diagnostic approach pairs rapid target screens with deep immune-context profiling to enable smarter therapy selection.
Closing the practical workflow gap: a pragmatic framework
To turn insights into action, implement a two-tier diagnostic framework: (1) reflex Target Verification (RTV) through repeatable IHC or targeted sequencing for promising alterations; and (2) Immune Contexture Mapping (ICM) using multiplex panels to quantify PD-L1, PD-1, T-cell subsets, and microenvironmental drivers. Real-world scenarios help clarify decisions:
- MEK1-high + PD-1+ T-cells: combine MEK inhibition with PD-1 blockade to potentially enhance cytotoxic activity while dampening immune escape.
- HER2-high + inflamed microenvironment: consider immunomodulatory partners beyond PD-1 blockade to overcome non-canonical resistance pathways.
- PD-L1+/PD-1- patterns: interpret cautiously; may imply alternative suppressive mechanisms or timing considerations for ICIs.
Implementation checklist and nested decision trees help clinicians operationalize the framework. The emphasis remains on aligning driver alterations with the immune milieu to anticipate resistance and optimize durable responses.
- Establish a reflex testing protocol with predefined targets based on local prevalence.
- Incorporate multiplex profiling at the reflex test result stage to capture immune contexture.
- Tag patients to signaling-immune phenotype buckets for trial stratification.
- Reflex testing yield: 40–60% more actionable cases than IHC alone
- Turnaround time: target ≤14 days for RTV; ≤21 days for ICM
- MEK1-driven tumors with PD-1+ T-cells: trial-ready combination.
- HER2-dominant cases: seek alternatives to PD-1 monotherapy.
Overall, the workflow should be standardized, scalable, and harmonized across centers to reduce variability and improve predictive accuracy for NSCLC patients considering targeted-immunotherapy regimens.
Mid-article data synthesis: a visual map
- Quadrant A: High PD-L1, high T-cell infiltration – good candidate for ICIs alone or with modest targeted agents.
- Quadrant B: Low PD-L1, high MEK1 signaling – consider MEK inhibition with ICI to unlock immune visibility.
- Quadrant C: High HER2, sparse T-cells – immunomodulatory backbone needed beyond PD-1 blockade.
Implementation checklist
- Adopt a two-step diagnostic workflow (IHC screening → reflex multiplex profiling).
- Define phenotype buckets that fuse driver data with immune contexture.
- Design trials with stratification by both target expression and immune state.
- Invest in cross-lab standardization for panels and interpretation rules.
What is the value of combining reflex testing with multiplex profiling in NSCLC?
Combining reflex testing with multiplex profiling provides a structured, evidence-based pathway to identify not only actionable targets but also the surrounding immune context that shapes response to therapy. This two-tier approach improves the accuracy of predicting which patients will benefit from targeted therapies alone, immunotherapies alone, or their combinations. It also helps avoid unnecessary exposure to ineffective drugs by clarifying whether a tumor is driven by a target pathway, an immune-suppressive milieu, or a combination of both. In practice, this means more precise selection for trials and standard-of-care regimens with higher probabilities of durable benefit.
From a clinical perspective, the combination supports a dynamic decision framework that accommodates tumor heterogeneity and resistance trajectories, enabling smarter sequencing and partner choices for NSCLC patients.
How should clinicians interpret PD-L1 in the context of MEK1 or EGFR signaling?
PD-L1 expression often coexists with other pathway activations such as MEK1, EGFR, or cMET, suggesting that the tumor may leverage multiple signaling axes to modulate the immune environment. Clinicians should interpret PD-L1 alongside pathway activation profiles rather than in isolation, as this integrated view can reveal whether combining checkpoint inhibitors with targeted agents may yield synergistic effects or, conversely, lead to antagonism. The goal is to align checkpoint status with actionable drivers to optimize combination strategies and patient outcomes.
What practical steps constitute reflex testing in routine NSCLC care?
Reflex testing begins with an initial rapid screen (IHC or targeted sequencing) to flag potential targets. If a target shows compelling, but not definitive, evidence of actionability, the pathway proceeds to multiplex profiling to map immune contexture and co-activated pathways. This two-step approach reduces false positives from single-marker tests and improves the likelihood that subsequent therapies address both tumor-intrinsic drivers and immune-extrinsic barriers.
What are typical scenarios where MEK inhibitors plus ICIs may be considered?
In tumors with MEK1 activation and substantial CD8+ T-cell infiltration, combining MEK inhibition with PD-1 blockade may enhance T-cell function and reduce immune resistance. However, the benefit likely depends on the balance of effector and regulatory populations, PD-1/PD-L1 expression levels, and the presence of co-activating targets. Clinicians should use multiplex contexture maps to identify patients whose tumors show this convergent signaling state and are most likely to respond to the combination.
How can trials be designed to reflect these biomarker combinations?
Trials should stratify participants by both target expression and immune contexture, ensuring balanced arms for MEK-enabled and non-MMEK strategies, with predefined immune readouts (PD-L1, PD-1, CD8, FoxP3) to monitor impact on response and resistance. Incorporating adaptive features enables dose and partner adjustments based on interim immune signals, accelerating the identification of durable, biomarker-informed regimens for NSCLC.
What microdata applies to FAQ optimization here?
The FAQ schema below supports search engines in surfacing concise, relevant responses to user queries. It links questions to explicit, evidence-backed explanations across target therapy, immunotherapy, reflex testing, and immune contexture, enabling better visibility for clinicians and patients seeking guidance on NSCLC biomarker strategies.






Add a comment
To comment, you need to register and authorize
Comments